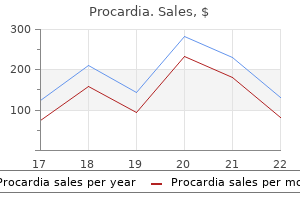
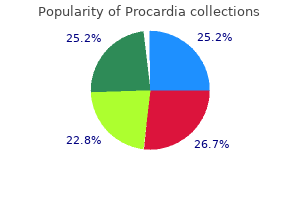
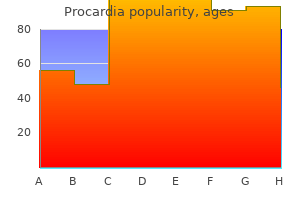
Procardia
"Order 30 mg procardia with amex, cardiovascular disease social justice principles".
B. Brontobb, M.A.S., M.D.
Co-Director, Stony Brook University School of Medicine
Most patients die inside a yr of prognosis cardiovascular thrombotic events procardia 30 mg order, however surgical resection of a solitary metastasis could additionally be healing capillaries lined with phagocytes procardia 30 mg with amex. Hematologic abnormalities heart disease meal plan cheap 30 mg procardia overnight delivery, together with pancytopenia and hemolytic anemia, are sometimes outstanding and in many instances due to splenomegaly from noncirrhotic portal hypertension. Lymphocytes often adhere to the endothelium of terminal venules and small branches of the portal veins, with or without subendothelial inflammation (endothelialitis). These small bile ducts are progressively destroyed, causing persistent cholestasis, the end stage of which is continual ductopenic rejection or Metastatic Cancer Is the Most Common Malignancy in the Liver Of all metastatic cancers, 1/3 have an result on the liver, including half of of cancers of the gastrointestinal tract, breast and lung. Pancreatic carcinoma, malignant melanoma and hematologic malignancies additionally often metastasize the liver, but any tumor might achieve this. The minimize surface of the liver exhibits many agency, pale lots of metastatic colon cancer. A portal tract is expanded by a polymorphous inflammatory infiltrate consisting of huge and small lymphocytes, plasma cells, macrophages, neutrophils and eosinophils. The gallbladder wall is composed of a mucous membrane, a muscularis and an adventitia. The mucosa is thrown into folds and consists of columnar epithelium and a lamina propria of unfastened connective tissue. Rokitansky-Aschoff sinuses are mucosal diverticula that dip into the gallbladder wall. Multiple cysts may happen as segmental dilations in the complete extrahepatic biliary tree. Similar multiple dilations in the intrahepatic biliary tree, referred to as Caroli illness, predispose to bacterial cholangitis. In the industrialized countries, 3/4 of gallstones are primarily ldl cholesterol; the remainder are calcium bilirubinate and different calcium salts (pigment gallstones). The cystic duct is about three cm lengthy and drains the gallbladder into the hepatic duct. Subintimal foam cells, intimal sclerosis and myointimal hyperplasia nearly obliterate the lumen of a hepatic artery. Obesity increases hepatic ldl cholesterol secretion much more, additional supersaturating the bile with ldl cholesterol. Local factors in the gallbladder: Bile in the gallbladder from sufferers with gallstones crystallizes more easily than normal. Biliary proteins can operate as nuclei of crystallization, and hypersecretion of gallbladder mucus accelerates cholesterol precipitation from gallbladder bile. Gallbladder motility: Impaired gallbladder motor perform leads to stasis causing bile sludging, which progresses to macroscopic stones. They are sometimes asymptomatic but cause delicate to severe ache (biliary colic) if they lodge within the cystic or widespread bile ducts. Estrogens increase hepatic secretion of cholesterol and decrease secretion of bile acids, perhaps explaining why ladies kind ldl cholesterol gallstones more usually. Progesterone, the principle hormone of pregnancy, inhibits discharge of bile from the gallbladder. The gallbladder empties more slowly, and the ensuing stasis increases the opportunity for cholesterol crystals to precipitate. Similar mechanisms may also explain the increase in gallstones with oral contraceptive use. Other main threat factors for ldl cholesterol gallstones embrace elevated biliary ldl cholesterol secretion, decreased secretion of bile salts and lecithin or both. Premenopausal women develop ldl cholesterol gallstones thrice more often than do men. The incidence is highest in users of oral contraceptives and ladies with several pregnancies. Cholesterol gallstones are quite common in Pima Indian ladies of the American Southwest; 75% are affected by age 25 years and 90% by age 60. In people who find themselves overweight, the relative danger of gallstones could additionally be fivefold above normal. Hepatic ldl cholesterol synthesis is stimulated by insulin, and the hyperinsulinism that accompanies elevated physique fats could clarify why biliary excretion of cholesterol increases with obesity. Decreased secretion of bile salts and lecithin happens in nonobese whites who develop gallstones. Cholesterol synthesis is elevated and bile salts and lecithin are lower in Pima Indians and in individuals taking sure medication. Moderate alcohol intake lowers biliary cholesterol concentration and decreases the chance of gallstones. The gallbladder has been opened to reveal quite a few small, darkish stones composed of calcium bilirubinate. Chronic hemolysis, as in hemoglobionopathies, predisposes to development of black pigment stones. Either because it will increase hemolysis or because of damage to liver cells, cirrhosis is also associated with a high incidence of black stones. Unconjugated bilirubin is insoluble in bile and is normally present in only trace quantities. If increased unconjugated bilirubin is secreted by hepatocytes, it precipitates as calcium bilirubinate, probably around a nidus of mucinous glycoproteins. Patients with out known predisposing components who develop black pigment stones have increased concentrations of unconjugated bilirubin within the bile for unknown causes. The rare circumstances in Western countries are seen in sufferers with persistent mechanical obstruction to bile flow, as in sclerosing cholangitis, or the presence of a catheter in the widespread bile duct after widespread bile duct surgical procedure. Bacterial -glucuronidase or different hydrolytic enzymes hydrolyze conjugated bilirubin to its unconjugated type, which favors formation of brown stones. The 15-year cumulative likelihood that asymptomatic stones will lead to biliary pain or other complications is less than 20%. Most issues of cholelithiasis relate to gallstones obstructing the cystic or widespread bile ducts. Passage of a stone into the cystic duct usually, but not always, causes extreme biliary colic and will lead to acute cholecystitis. Repeated bouts of acute cholecystitis give rise to chronic cholecystitis, which can also result from the presence of stones alone. Gallstones coming into the widespread duct (choledocholithiasis) might cause obstructive jaundice, cholangitis and pancreatitis. Passage of a giant gallstone into the small gut can even trigger intestinal obstruction, generally identified as gallstone ileus. Gallbladder removed from a patient with acute cholecystitis demonstrates ulceration of the mucosa (left) and acute and continual inflammation. The lumen of the dilated gallbladder is full of clear mucus and contains ldl cholesterol stones. Rarely, in empyema of the gallbladder, the cystic duct is completely obstructed, allowing micro organism to invade the gallbladder and distending the organ with cloudy, purulent fluid. The mucosa shows focal ulcers or, in extreme instances, widespread necrosis (gangrenous cholecystitis). More typically, inflammatory adhesions type a pericholecystic abscess and limit unfold of gallbladder contents after perforation. Erosion of gallbladder contents into a viscus might create a cholecystenteric fistula. It is almost all the time associated with gallstones but may also result from repeated attacks of acute cholecystitis. In the latter case, the pathogenesis most likely relates to persistent irritation and chemical damage to the gallbladder epithelium. The remaining instances (acalculous cholecystitis) are linked to sepsis, severe trauma, infection of the gallbladder with Salmonella typhosa and polyarteritis nodosa. Bacterial an infection is often a consequence of biliary obstruction quite than a main event. Obstruction of the cystic duct by a gallstone could lead to launch of phospholipase by the gallbladder epithelium. The mucous coat of the epithelium is disrupted, exposing mucosal cells to the detergent action of concentrated bile salts. Mild jaundice, attributable to stones in, or edema of, the common bile duct, is seen in 20% of patients. The acute illness generally subsides inside per week, however persistent ache, fever, leukocytosis and shaking chills herald development of the disease and the necessity for cholecystectomy. As inflammation resolves, the gallbladder wall becomes fibrotic and the mucosa heals.
Worldwide cardiovascular disease smoking procardia 30 mg cheap without a prescription, the most common lymphomas are follicular lymphoma (29%) and diffuse large cell lymphoma (37%) blood vessels quiz game buy procardia 30 mg low price, exclusive of Hodgkin lymphoma and plasma cell myeloma (Table 26-20) cardiovascular x-ray procardia 30 mg order on-line. A variant of diffuse large B-cell lymphoma, mediastinal giant B-cell lymphoma, is an exception, with a median age of 35. Mature B-cell lymphomas, apart from Burkitt and diffuse massive B-cell lymphomas, are distinctly uncommon in kids. Risk factors for growth of B-cell lymphoma embrace abnormalities of the immune system. Presenting white blood cell counts are normally excessive, and a mediastinal mass or other tissue mass (lymphoma) is often current. The tumor normally grows rapidly, and sufferers with mediastinal involvement may current with respiratory misery due to compression of the central airways or superior vena cava syndrome. Mature B-Cell Lymphomas Are the Most Common Type of Lymphoma in the Western World Mature B-cell malignancies are clonal proliferations of differentiated B cells. Their habits usually reflects their morphology, immunophenotype, genetic lesions and clinical presentation (including stage). Low-grade B-cell lymphomas tend to develop in patients with certain autoimmune ailments. Large activated B cells (centroblasts) residence to germinal centers where they mature into smaller cells with cleaved nuclei (centrocytes). Follicular lymphomas derive from germinal heart B cells and contain a mix of centroblasts and centrocytes that overexpress Bcl-2, which provides them a survival advantage. Burkitt lymphoma and a few diffuse large B-cell lymphomas additionally come from germinal center lymphocytes, with the latter often identified as germinal center�type B-cell lymphomas. Late-stage reminiscence B cells reside in marginal zones, the outermost compartment of lymphoid follicles. The latter, notably, involve extranodal websites such as the abdomen and different mucosal tissues. These are the only B cells to secrete antibodies, although they lack detectable cell surface immunoglobulins. Plasma cells residence to the bone marrow, where they could give rise to multiple myeloma. The latter represents an important exception to the overall rule of small cell morphology predicting indolent conduct (see below). In contrast, aggressive lymphomas progress rapidly, however many are curable with standard therapies. Its overall annual incidence is 2�6 circumstances per 100,000 folks, but the incidence will increase with age to 12. Cases with unmutated immunoglobulin segments are likely to behave extra aggressively, for unknown reasons. The nuclear chromatin is clumped and infrequently has a blotchy appearance resembling cracked mud; nucleoli are absent within the small cells. In addition to the small cells, all instances also have some bigger cells with spherical nuclear contours, much less condensed chromatin, and a single prominent central nucleolus; these cells are generally known as prolymphocytes within the blood, they usually usually account for less than 10% of whole lymphocytes. Large confluent sheets of paraimmunoblasts or different giant lymphoid cells could symbolize transformation to diffuse giant B-cell lymphoma (see below). Bone marrow involvement ranges from complete effacement of the marrow area to patchy interstitial or nonparatrabecular infiltrate of varying degree. Gross picture of a bisected, enlarged lymph node exhibits the attribute uniform, glistening, fish-flesh appearance seen in tissues concerned by lymphoma. A smear of peripheral blood reveals quite a few small to medium-sized lymphocytes with clumped nuclear chromatin. On microscopic examination, the nodal structure is replaced by a diffuse proliferation of small lymphocytes admixed with a low variety of larger cells generally identified as paraimmunoblasts (arrows) present in scattered proliferation centers. Often the primary hint of the disease is an abnormal full blood depend displaying absolute lymphocytosis. Flow cytometry of the peripheral blood is adequate to set up the analysis in most cases. The different peripheral counts could also be normal or irregular, and findings corresponding to platelet rely and hemoglobin stage are used to stage the illness. Erythrocyte and platelet counts are initially normal, however as the illness advances, severe anemia, thrombocytopenia and even neutropenia can develop. A constructive Coombs test occurs through the course of disease in up to 20% of sufferers and may be related to immune-mediated hemolytic anemia. A small monoclonal paraprotein may be present in some sufferers, most of which are of the IgM heavy-chain type (in distinction to sufferers with multiple myeloma, who most frequently have IgG paraproteinemias). Hypogammaglobulinemia occurs in 50%�75% of instances in some unspecified time within the future in the course of the illness; the diploma of hypogammaglobulinemia usually correlates with disease stage and is answerable for infectious complications. The T cells, although increased in quantity, typically present impaired delayedtype hypersensitivity reactivity, which may contribute to the increased danger of an infection. For occasion, patients with low disease burden can survive over 10 years, whereas others with extensive illness or poor prognostic options present rapid development and will not survive greater than 2 or 3 years. Transformation to prolymphocytic leukemia occurs in 15%�30% of circumstances and is the commonest form of development. This type of transformation is heralded by worsening cytopenias, increasing splenomegaly and progressive increases in prolymphocytes in the blood or paraimmunoblasts in lymph nodes or other tissues. Transformation to diffuse large B-cell lymphoma, Richter syndrome, happens in 10% of circumstances. This form of development is marked by the looks of a rapidly enlarging mass, worsening of systemic signs and a excessive lactate dehydrogenase degree in the serum. Other rare forms of transformation additionally happen, together with a Hodgkin lymphoma or Hodgkin-like transformation, the latter occurring more regularly in patients treated with certain chemotherapeutic drugs. Most patients who undergo prolymphocytic or Richter transformation survive less than 1 12 months. The neoplastic cells are heterogeneous, with a mix of small and enormous cleaved cells and centroblasts. This largely displays the histologic grade, which depends on the number of centroblasts in the neoplastic follicles. It solely hardly ever occurs in individuals underneath age 20, and is extra widespread in women than males. It puts expression of the antiapoptotic protein, Bcl-2, under control of the IgH promoter, and ends in Bcl-2 overexpression. Bcl-2 protein is an inhibitor of apoptosis and offers a survival advantage to the lymphoma cells. The neoplastic follicles are present in excessive density, and are often in a back-to-back association with little intervening paracortex. The neoplastic follicle centers (germinal centers) comprise a mix of small and enormous cells with irregular nuclear contours (centrocytes/cleaved cells) and scattered centroblasts, which have round nuclear contours and a quantity of nucleoli connected to the nuclear membrane. The normal lymph node architecture is replaced by malignant lymphoid follicles in a back-to-back sample. Malignant lymphoid follicle germinal centers may be distinguished from normal/reactive germinal centers utilizing immunohistochemistry for Bcl-2. Circulating follicular lymphoma cells are current in the blood in 10% of circumstances; they present prominent nuclear irregularity and deep nuclear clefts. Extranodal presentations are relatively uncommon, in comparison with different B-cell lymphomas. The lymphadenopathy is painless and may have followed a waxing and waning course earlier than the patient seeks medical consideration. As discussed above, the medical course is linked to histologic grade, and progression/transformation to extra aggressive disease could occur in 50% of instances. The neoplastic follicles are composed of predominantly small cleaved cells (centrocytes) and only a few scattered centroblasts are present. The neoplastic follicle shows a mix of small and huge cleaved cells and centroblasts characterized by a number of nucleoli (arrows). The neoplastic follicle exhibits a predominance of centroblasts with solely uncommon admixed centrocytes. The persistence of a follicular pattern helps distinguish this entity from diffuse giant B-cell lymphoma. Cyclin D1 drives cell cycle development on the G1-to-S-phase transition, by binding to Cdk4/6.
A somatotroph adenoma arising before epiphyses shut in a baby or adolescent causes gigantism coronary artery lcx procardia 30 mg buy cheap on-line. After lengthy bone epiphyses have fused and grownup height has been attained cardiovascular system video lecture effective 30 mg procardia, nonetheless capillaries quizlet order procardia 30 mg fast delivery, the identical tumor produces acromegaly. Most tumors are macroadenomas and cause mass results and tumor-induced adenohypophyseal hypofunction. Pituitary macroadenomas may compress the optic chiasm, causing severe headaches, bitemporal hemianopsia and lack of central imaginative and prescient. Large adenomas could invade the hypothalamus, intervene with regular hypothalamic enter to the pituitary and lead to lack of temperature regulation, hyperphagia and hormonal syndromes. Sparsely granulated adenomas have small chromophobe cells with characteristic spheroid cytoplasmic inclusions, called "fibrous our bodies," that contain keratin intermediate filaments, particularly keratin 8. Acidophil stem cell adenomas are monomorphous, slightly acidophilic tumors with nuclear pleomorphism and large cytoplasmic vacuoles. Key options embrace big mitochondria, keratin 8�positive fibrous our bodies and misplaced exocytosis. Most acromegalics have neurologic and musculoskeletal signs, together with headaches, paresthesias, arthralgias and muscle weak spot. One third have hypertension, and even half of normotensive acromegalics have elevated left ventricular mass and are in danger for congestive coronary heart failure. Diabetes happens in up to 20%, and hypercalciuria and renal stones develop in another 20%. Half of acromegalics have hyperprolactinemia extreme sufficient to be symptomatic (see above). A few useful corticotroph adenomas are chromophobic and extra aggressive than their basophilic counterparts and should show pleomorphic features and apoptosis. By electron microscopy, basophilic adenomas contain many secretory granules and perinuclear bundles of nice, keratin-positive, intermediate filaments (type I filaments). They come to medical attention when there are signs of hyperthyroidism, goiter or a pituitary mass lesion. Thyrotroph adenomas are predominantly macroadenomas and could be invasive and fibrotic. They are chromophobic, with polyhedral or columnar cells that type collars round blood vessels. By electron microscopy, secretory granules are often organized in a single row just subjacent to the plasma membrane. Patients with long-standing hypothyroidism could develop hyperplasia of pituitary thyrotrophs (thyroid deficiency cells), presumably as a outcome of insufficient feedback inhibition by thyroid hormones. They are slowly rising macroadenomas that happen in older people and come to medical attention because of their mass effect. Tumor cells are negative or sparsely optimistic for all anterior pituitary hormones. Oncocytomas are variants of nonfunctional null cell adenoma, containing enlarged, eosinophilic and often granular cells. The neoplastic cells of oncocytomas are filled with mitochondria but are in any other case much like different null cell adenomas. Silent adenomas differ from different nonfunctional pituitary adenomas in showing nicely differentiated ultrastructurally. Currently, there are over 35 mutations known in familial neurohypophysial diabetes insipidus. Mutations or deletions within the vasopressin V2 receptor (Xq28) and the vasopressinsensitive aquaporin-2 water channel genes might trigger nephrogenic diabetes insipidus. The hypothalamus may be damaged by main and metastatic tumors, viral infections and granulomatous inflammations, in addition to degenerative and hereditary disorders. Hypothalamic dysfunction can also occur with out an identifiable anatomic abnormality. Diverse situations result from disturbances of hypothalamic perform and include, amongst others, hypogonadism, precocious puberty, amenorrhea and eating disorders (obesity or anorexia). Some pituitary problems characterized by increased or decreased hormone secretion have their origin in hypothalamic dysfunction. Coronal part of the mind reveals a big, cystic tumor mass changing the midline constructions within the area of the hypothalamus. The primitive thyroid descends to its eventual location in the lower anterior neck by elongation of its tubular attachment to the tongue, the thyroglossal duct, which then atrophies across the seventh week of life. The adult thyroid has two lobes related by an isthmus and is under the thyroid cartilage anterior to the trachea. In its early improvement, the gland accommodates cords of cells that will turn into the follicles or acini that make up the useful items of the thyroid gland. Follicles common 200 m and are formed by a single row of cuboidal cells surrounded by a fragile basement membrane. These are provided by a lobular artery and sustained by a diffuse mesh of fibrous stroma, lymphatics and connective tissue. This substance represents secreted thyroglobulin, from which active thyroid hormones are released. Immunohistochemical staining for thyroglobulin has turn into a robust marker to determine follicular cells. In addition to follicular epithelial cells, the thyroid additionally incorporates parafollicular or C cells in the lateral elements of the higher portion of each thyroid lobes, near the follicles. They produce calcitonin, a calciumlowering hormone, and can also secrete smaller amounts of different peptides corresponding to serotonin and somatostatin. C cells are tough to determine using routine stains however are readily seen by immunostaining for calcitonin or neuroendocrine markers such as chromogranin and synaptophysin. Trauma and hypophysectomy for anterior pituitary tumors account for most remaining circumstances of diabetes insipidus. Less often, localized hemorrhage or infarction, Langerhans cell histiocytosis (see Chapter 26) or granulomatous infiltrates involve the posterior pituitary stalk or body. Polyuria could additionally be managed by powdered posterior pituitary or vasopressin given as snuff. The cysts can be lined by squamous or respiratory-type epithelium and contain variable amounts of thyroid tissue. Surgical excision is healing, and portions of the hyoid bone ought to be removed to keep away from recurrences. Alone among endocrine glands, the thyroid can store a appreciable quantity of preformed hormone. On demand, follicular cells reabsorb thyroglobulin, liberate T4 and T3 by proteolytic cleavage and launch them into the blood. Most secreted hormone is T4, which is deiodinated in peripheral tissues to its extra lively kind, T3. Peripheral cells take up only free hormone, which binds to nuclear receptors and initiates particular protein synthesis. It stimulates basal metabolic price and metabolism of carbohydrates, lipids and proteins. It increases body heat and hepatic glucose manufacturing by rising gluconeogenesis and glycogenolysis. Glucose use, fatty acid synthesis within the liver and adipose tissue lipolysis all increase. In common, thyroid hormone upregulates overall metabolic activities, both anabolic and catabolic. Nontoxic goiter (from the Latin, guttur, "throat"), also referred to as easy, colloid or multinodular goiter or nodular hyperplasia, is thyroid enlargement without useful, inflammatory or neoplastic adjustments. Diffuse goiter is frequent in adolescence and through being pregnant, whereas the multinodular type usually happens in people older than 50 years. In unhazardous goiter, the capacity of the thyroid to produce thyroid results in enlargement of the gland, which maintains the euthyroid state. Such ectopic thyroid tissues are functionally normal and can produce thyroid hormone. Ectopic thyroid tissue may occur in lymph nodes and delicate tissue adjacent to the normal gland. Some hold that each one of these circumstances actually characterize welldifferentiated metastases from occult thyroid cancers; others see them as embryonal rests lateral to the thyroid. If the aberrant thyroid tissue is histologically malignant (see below), then the lesion must be thought of a metastasis. This occurs more in females and normally is found because of problem in swallowing, talking or respiratory.
Thromboembolus within the left anterior descending coronary artery of a man who had old rheumatic coronary heart illness coronary heart procedure buy generic procardia 30 mg line, mitral stenosis and a mural thrombus within the left atrial appendage capillaries and venules procardia 30 mg fast delivery. Extensive collateral connections develop in hearts with severe coronary atherosclerosis blood vessels that return blood to the heart generic procardia 30 mg visa. These collaterals may very well present sufficient arterial circulate to forestall infarction completely or to restrict infarct size when a serious epicardial coronary artery is acutely occluded. Well-developed coronary collaterals can clarify sure uncommon situations, such as anterior infarction after recent thrombotic occlusion of the best coronary artery (so-called infarction at a distance). Acute thrombosis of the right coronary artery might then cause paradoxical infarction of the anterior left ventricular wall. Conditions that increase blood stress or cardiac output, such as exercise or being pregnant, improve myocardial demand, which may result in angina pectoris or infarction. Hyperthyroid sufferers have increased metabolic charges and tachycardia, resulting in elevated oxygen demand and higher cardiac workload. Treatment of the underlying thyroid disease is the best therapy for a hyperthyroid patient with signs of cardiac ischemia. It may come up inside the territory of one of the major epicardial coronary arteries or it might be circumferential, involving subendocardial distributions of multiple coronary arteries. It may be as a outcome of atherosclerosis in a single coronary artery or because of ailments that restrict myocardial blood circulate globally, similar to aortic stenosis, hemorrhagic shock or hypoperfusion throughout cardiopulmonary bypass. Because necrosis is restricted to the inside layers of the guts, complications arising in transmural infarcts. Coronary arteritis occurs in numerous vasculitides, such as polyarteritis nodosa or Kawasaki disease. Rarely, medial necrosis and dissecting aneurysms are restricted to a coronary artery. Syphilitic aortitis characteristically affects the ascending aorta, the place it could obliterate a coronary artery orifice. Congenital anomalous origin of a coronary artery (origin of a coronary artery from the pulmonary trunk or passage of an anomalous coronary artery between the aorta and pulmonary artery) might trigger sudden death in young, in any other case wholesome individuals. The artery normally runs within the epicardial fats, however in some hearts, it dips into the myocardium for a brief distance. The muscular bridge might compress the artery during systole or predispose to coronary spasm. A transmural infarct involves the total left ventricular wall thickness, usually after occlusion of a coronary artery. Macroscopic Characteristics of Myocardial Infarcts the early phases of myocardial infarction have been characterized most thoroughly in experimental animals. Within 10 seconds after ligation of a coronary artery, the affected myocardium turns into cyanotic and, quite than contracting, bulges outward during systole. This reversible stage lasts for 20�30 minutes of complete ischemia, after which broken myocytes progressively die. By 2�3 weeks, the infarcted area is depressed and soft, with a refractile, gelatinous look. Left circumflex coronary artery: Obstruction of this vessel is the least common explanation for myocardial infarction, inflicting infarcts of the lateral left ventricle wall. Rather, it first develops within the subendocardium and progresses as a wavefront of necrosis from subendocardium to subepicardium over a quantity of hours. Transient coronary occlusion may cause only subendocardial necrosis, but persistent occlusion eventually results in transmural necrosis. The objective of acute coronary interventions (pharmacologic or mechanical thrombolysis) is to interrupt this wavefront and limit myocardial necrosis. The volume of arterial collateral circulate is the chief determinant of transmural development of an infarct. In persistent cardiac hypoperfusion, intensive collaterals, which preferentially provide the outer or subepicardial layer, usually restrict infarction to the subendocardial myocardium. However, in deadly cases, acute transmural infarcts are extra widespread than those restricted to the subendocardium. Infarcts involve the left ventricle much more usually and extensively than the best ventricle. This difference may be partly defined by the higher workload imposed on the left ventricle by systemic vascular resistance and the higher thickness of the left ventricular wall. Infarction of the posterior right ventricle happens in a couple of third of left ventricular posteroseptal infarcts (right coronary artery territory), however infarcts restricted to the proper ventricle are rare. A cross-section of the guts from a person who died after an extended history of angina pectoris and several other myocardial infarctions shows near-circumferential scarring of the left ventricle. Electron micrograph of an irreversibly injured myocyte from a canine heart subjected to 40 minutes of low-flow ischemia induced by proximal occlusion of the circumflex branch of the left coronary artery. The mitochondria (M) are additionally swollen and include amorphous matrix densities (amd), that are attribute of deadly cell damage. The chromatin of the nucleus (N) is aggregated peripherally, in distinction to the uniformly distributed chromatin in regular tissue. After about 12� 18 hours, the infarcted myocardium exhibits eosinophilia (red staining) in sections of the guts stained with hematoxylin and eosin. About 24 hours after the onset of infarction, polymorphonuclear neutrophils infiltrate necrotic myocytes at the periphery of the infarct. After about 3 weeks, peripheral parts of the infarct are composed of granulation tissue with outstanding capillaries, fibroblasts, lymphoid cells and macrophages. The necrotic particles has been largely faraway from this space, and a small quantity of collagen has been laid down. Reversibly injured myocytes present delicate changes of sarcoplasmic edema, gentle mitochondrial swelling and loss of glycogen (the ultrastructural correlates of stunned myocardium). After 30�60 minutes of ischemia, when myocyte harm has become irreversible, mitochondria are significantly swollen with disorganized cristae and amorphous matrix densities made from calcium phosphate salts shaped by huge Ca2+ overload in severely injured cells. Nuclei present clumping and margination of chromatin and the sarcolemma is focally disrupted. Ion gradients are also dissipated, and tissue potassium decreases as sodium, chloride and calcium increase. The noncontractile ischemic myocytes are stretched with each systole and turn out to be "wavy fibers. By 2�3 days, muscle cells are more clearly necrotic, nuclei disappear and striations turn into less outstanding. A part on the edge of a healed infarct stained for collagen, which appears blue-green here, reveals dense, acellular areas of collagenous matrix sharply demarcated from the adjoining viable myocardium. The periphery of the infarcted area exhibits phagocytosis of lifeless muscle by macrophages. The process of replacing necrotic muscle with scar tissue starts at about 5 days, first on the edge of the infarct, steadily transferring inward. This sequence of inflammatory and reparative occasions can be altered by local or systemic factors. For example, instant extension of an infarct into a region that beforehand had patchy necrosis may not show anticipated adjustments. However, blood move may be restored to areas of evolving infarcts both due to spontaneous thrombolysis or in response to therapeutic opening of occluded coronary arteries. Reperfused infarcts are usually hemorrhagic, from blood flow via broken microvasculature. Thus, infarcts after persistent occlusion are only grossly obvious after about 12 hours and are pale, but hemorrhage instantly highlights reperfused infarcts. The necrotic myocardial fibers, which are eosinophilic and devoid of cross-striations and nuclei, are immersed in a sea of acute inflammatory cells. These "clinically silent" infarcts are particularly common among diabetics with autonomic dysfunction and in cardiac transplant sufferers whose hearts are denervated. A part of infarcted myocardium reveals distinguished, thick, wavy, transverse bands in myofibers. Complications of Myocardial Infarction the infarct, somewhat than solely on the periphery. Replacement of necrotic muscle by fibrous scar also happens more shortly, a minimal of in areas of the infarct by which perfusion persists. One of probably the most attribute options of reperfused infarcts is contraction band necrosis. By electron microscopy, these bands are small teams of hypercontracted and disorganized sarcomeres with thickened Z disks. The sarcolemma is disrupted and mitochondria positioned between the contraction bands swell.
The sinuses are lined by macrophages cardiovascular system gif discount 30 mg procardia overnight delivery, which are concerned in antigen presentation (see Chapter 4) blood vessels model generic procardia 30 mg with mastercard. The arrangement of the sinuses maximizes publicity to foreign antigens present within the lymph to macrophages and immunoreactive lymphocytes within the lymph nodes artery 30 mg procardia generic with amex. The cortex is subdivided into a follicular space (which contains mostly B cells) and a paracortical area (predominantly T cells, plus many postcapillary venules). Lymphocytes from the circulation enter the lymph node cortex by migrating through the tall endothelial cells of the postcapillary venules within the paracortex. T cells are most likely to remain within the paracortex, while B lymphocytes house to the follicle germinal centers. The B-cell�rich cortex accommodates two forms of follicles: (1) immunologically inactive follicles, referred to as main follicles; and (2) immunologically lively follicles, called secondary follicles. Primary follicles are cohesive aggregates of small lymphocytes with out well-defined germinal facilities or mantle zones. Secondary follicles include germinal facilities in which giant noncleaved lymphocytes (centroblasts) mingle with small and larger lymphocytes with cleaved nuclei (centrocytes). Macrophages, and to a lesser extent dendritic cells, present development elements for activated B cells. The T-cell�rich paracortex, also called the deep cortex or parafollicular area, is both between the B-cell follicles and deep to them. Hematogones enhance in number throughout viral infections and in bone marrow restoration after chemotherapy or stem cell transplantation. A fraction of the bone marrow-derived progenitor B cells leave the marrow and home to lymph node germinal facilities, where additional development and selection happens. Specifically, B cells with enough affinity for antigen survive the germinal middle reaction and finally leave the follicle compartment. As B lymphocytes mature, the genes for Ig heavy (H) chains are rearranged, leading to the synthesis of IgM antibodies. After activation and clonal growth on this entity is typically called a chloroma because of its greenish color, granulocytic sarcoma or monoblastic sarcoma. Lymphocytes in tonsils and Peyer patches arrive in these websites by migration through the tall endothelial cells of vessels, that are similar to the postcapillary venules in lymph nodes. B cells undergo activation, transformation and selection in the lymph nodes and spleen. All lymphocyte improvement entails a tightly managed sequence of gene expression and silencing that leads to sequential gain and lack of nuclear material and modifications cytoplasmic and/or floor antigen expression. Patterns of antigenic expression determine the lineage and maturation stage of normal and neoplastic lymphoid cells (see under and Chapter 4). Larger nodes are thought of clinically enlarged and could additionally be abnormal microscopically. Sometimes many nodes within a series or group could also be enlarged and/or matted together, usually a feature of malignancy. There, they become Ig-secreting plasma cells, or they exit the lymph nodes as memory B cells. Plasma cells have eccentric nuclei with clumped chromatin marginated at the nuclear membrane, historically described as "clock-face chromatin. Recombination of T-cell receptor genes generates a diverse inhabitants of T cells, every of which might acknowledge a single antigen. Once mature and educated, T cells leave the thymus to lymph nodes, spleen and peripheral blood to turn out to be postthymic T cells. The antigens presented to T-helper cells are peptide fragments derived from partial digestion of international proteins by macrophages and/or different antigen-presenting cells. The T-helper cells in turn work together with B lymphocytes that specific the identical antigenic specificity and induce the latter to proliferate and differentiate into plasma cells. Lymphocytes have various morphologies in stained peripheral blood and bone marrow smears, as nicely as in tissue sections. Like other blast cells, immature lymphoid cells have excessive nuclear-to-cytoplasmic ratios, fantastic chromatin and visual nucleoli. Following the lymphoid stem cell and precursor stage within the bone marrow, B cells mature into naive B lymphocytes and home to the secondary lymphoid organs (primarily lymph nodes). The germinal-center response represents an important turntable for immunoglobulin variable-region gene mutations, Ig heavy-chain switch and differentiation into plasma cells and memory B cells. B-cell immunoblasts and plasmacytoid immunoblasts reside within the T-cell�rich paracortex and medulla, respectively. In peripheral blood smears, transformed cytotoxic T cells are variant lymphocytes (sometimes called "atypical lymphocytes"). Variant lymphocytes tend to have plentiful blue-gray cytoplasm and multiple nucleoli in Wright-Giemsa�stained smears. The similar cells in tissue sections stained with hematoxylin and eosin have round to oval nuclei, one to several eosinophilic nucleoli apposed to their nuclear membranes and abundant clear to purple cytoplasm. Precise identification and characterization of lymphoid cells requires flow cytometric or immunohistochemical analysis. The time period "variant lymphocytes" covers atypical lymphocytes and large granular lymphocytes. Large granular lymphocytes are medium to massive lymphoid cells with some pink cytoplasmic granules. Plasmacytoid lymphocytes have abundant blue cytoplasm and are seen in some reactive issues. Bone marrow plasmacytosis greater than 10% is often associated with a plasma cell neoplasm. In each reactive and neoplastic plasma cell proliferations, immunoglobulin may accumulate within the cytoplasm to type outstanding eosinophilic globules, generally known as Russell our bodies. Similarly, benign and neoplastic plasma cells may comprise nuclear pseudoinclusions (Dutcher bodies), which symbolize immunoglobulin invaginated into the nucleus and seen in cross-section. Lymphocytopenia Usually Reflects a Decrease in T-Helper Lymphocytes Peripheral blood lymphocytopenia is outlined as a blood lymphocyte depend lower than 1500/L in adults or lower than 3000/L in children. An absolute lymphocytosis brought on by a heterogeneous population of small and bigger lymphoid cells, including atypical lymphocytes, is characteristic of this Ebstein-Barr virus� driven disorder. Other much less frequent causes of reactive lymphocytosis include pertussis, continual bacterial infections similar to tuberculosis and brucellosis, stress and cigarette smoking. Persistent absolute lymphocytosis, greater than 4000/L, notably in adults, raises suspicion for a lymphoproliferative disorder and deserves additional analysis. Decreased lymphocyte manufacturing: Several congenital and purchased immunodeficiency syndromes entail lowered technology of lymphocytes. Impaired T-cell manufacturing also happens with some lymphomas, similar to classical Hodgkin lymphoma, notably in superior phases. Loss of lymphocytes: Disorders related to harm to intestinal lymphatics can result in lack of lymph fluid and lymphocytes into the gut lumen. Such illnesses embrace protein-losing enteropathies, Whipple disease and circumstances of elevated central venous pressure. Immunologic harm to lymphocytes might occur in collagen vascular ailments, such as systemic lupus erythematosus. The histology and magnitude of lymph node enlargement in reactive hyperplasia are features of the age of the affected person (children are likely to present higher immunoreactivity than do adults), the immunologic competence of the host and the inciting stimulus. Acute suppurative and necrotizing lymphadenitis happens in lymph nodes that drain websites of acute bacterial or fungal infections. Such nodes enlarge rapidly because of edema and hyperemia, and are often tender as a result of the capsule turns into distended. Lymph node sinuses and stroma are infiltrated by neutrophils and variable numbers of bland macrophages. Well- or poorly outlined granulomas are frequent, and necrosis could be focal and Plasma cells in peripheral blood: It is unusual to find plasma cells in the blood. The presence of circulating plasma cells in the blood of an grownup raises suspicion for a plasma cell neoplasm, such as plasma cell myeloma (see below). Reactive bone marrow plasmacytosis: Plasma cells normally account for lower than 3% of hematopoietic cells in the bone marrow.
Buy generic procardia 30 mg on-line. 3 Exercises to Increase STAMINA - Endurance for a Fight.